Overview
The Hydrotherapy Center and Avène Thermal Spring Water are known for their soothing properties to treat skin concerns. In 1874, the French government declared them to be an official “public benefit.” In 1966, the Hydrotherapy Center was approved for reimbursement by the French Healthcare System and is available as a treatment for a variety of skin conditions.
Avène Thermal Spring Water (TSW) is characterized by a low mineral content. In vitro experiments have demonstrated the effect of TSW on membrane fluidity, its antiradical and anti-inflammatory properties, immunomodulatory, and its stimulating effect on keratinocyte differentiation.1 Additionally, a unique microorganism, Aquaphilus dolomiae, has been identified in thermal water, not yet described in other environments, thought to be responsible for significant pharmacological activities on inflammation, pruritus, and the strengthening of innate immunity.2
Atopic dermatitis (AD) has a complex, multifactorial pathophysiology, and an ever-growing list of associated cytokines.3 While several cytokines now have targeted therapies (ie, IL-4, IL-13, IL-31), there are numerous therapies in development for yet other cytokines and combinations, as well as broader approaches.4,5 Beyond inflammation, therapies may also address optimization of keratinocyte differentiation, itch, and increasing diversity of the skin microbiome.2
One observational study of patients treated at the hydrotherapy center in Avène diagnosed with either AD (n = 5916) or psoriasis (n = 4887) showed a significant improvement in SCORAD observed between Day 0 and Day 18 (−41.6%) (p < 0.0001) and similarly, a significant reduction in PASI was noted between Day 0 and Day 18 (−54.4%) (p < 0.0001) after 3-weeks of hydrotherapy. PASI 50 and PASI 75 were 64.3% and 19.5% respectively. For AD patients (n = 1102) or patients suffering from psoriasis (n = 833) who came for two consecutive years, a significant SCORAD and PASI improvement was observed on Day 0 of the second year when compared with Day 0 of the previous year (p < 0.0001).6
In a study of psoriasis patients with chronic pruritus, twenty-six underwent 3 weeks of hydrotherapy with a 3- and 6-month follow-up. A control group (18 patients) did not undergo hydrotherapy and continued to follow their usual skin management. Pruritus measurements (NRS, vDPS, and 5-D itch scale) indicated an immediate and long-lasting positive effect of hydrotherapy compared with control patients. In the hydrotherapy group, the mean pruritus intensity was more markedly decreased and was evident at the end of the 3-week hydrotherapy on Visit 2 (V2), an effect which was sustained over the remaining visits (the mean pruritus intensity was statistically significantly decreased (p = 0.0001) on V2, V3, and V4 compared with V1 by 50.4%, 53.4%, and 47.7%, respectively). The psoriasis area and severity index (PASI) scores were decreased by 40.0% with hydrotherapy, which was sustained over 6 months. The ItchQoL also improved directly after hydrotherapy, which was still much improved even 6 months later. Analysis of gene and/or protein biomarkers revealed a significant decrease of inflammation biomarkers (IL-8, IL-1α, IL-1RA, and RANTES), of psoriasis biomarkers (PI3, S100A7, and IL-17), and of pruritus biomarkers (IL-31, TRPV1, and CGRP1).7
The clinical efficacy of the water was demonstrated at the hydrotherapy center in chronic and disabling diseases such as AD but also in various medical settings as well as after-procedures such as photodynamic therapy or fractional laser resurfacing.8
A panel of US dermatologists convened at the hydrotherapy center in Avène, France to understand the patient benefit of the 3-week treatment utilizing the water from its natural source, used in-conjunction with specific postbiotic topical products for patients with inflammatory skin conditions. A primary objective was to come to a consensus on how therapy inspired by the Avène hydrotherapy treatment could be implemented utilizing both commercially available thermal spring water from the spring in Avène, and the same postbiotic skincare products as a standalone treatment and in conjunction with other conventional treatments.
Background
Chronic inflammatory immune-related skin disease’ (ISDs) is an umbrella term grouping heterogeneous entities characterized by chronic inflammation potentially involving the whole skin.9
The importance of discovering ways to implement to hydrotherapy treatments as an adjunctive therapy with the many treatment options available is underscored by the magnitude of the physical, emotional, quality of life, and economic toll of inflammatory skin conditions and the often-passionate patient opinions and concerns about the types of treatments they are both willing to receive and utilize at home.10–14
The Avène Hydrotherapy Center (Avène les Bains, France) provides hydrotherapy for various dermatological conditions. Treatment courses, which are prescribed and supervised by dermatologists in conjunction with hydrotherapists, massage therapist well as other specialists in nutrition and mental health. The treatment course lasts 3 weeks and involve various procedures (eg, baths, showers, sprays, underwater massages, and drinking the water) using the natural TSW, directly from the source without any additives. In addition to hydrotherapy, basic care at the Avène Hydrotherapy Center includes education about general health, skin health, diet, and nutrition while engaging with the natural surroundings.8
Therapeutic treatments at the center heavily feature the TSW with Aquaphilus dolomiae as well as Aquaphilus dolomiae-derived postbiotic skin care products. The comprehensive nature of the treatment at the hydrotherapy incorporates additional modalities and support services, most notably modified wet wrap therapy utilizing the TSW and postbiotic skin care. All adjunctive care support has potential for inclusion in protocols that can be leveraged away from the actual center and has documented benefits.
Wet Wrap Therapy: Wet wrap therapy (WWT) is one method to quickly reduce AD severity and is often utilized in the setting of significant flares and/or recalcitrant disease. It may be performed on an ambulatory or inpatient basis. WWT appears to help via occluding the topical agent for increased penetration, decreasing water loss, as well as providing a physical barrier against scratching. The wrap can be worn from several hours to 24 hours at a time, depending on patient tolerance. Most suggest several days of use, although a few studies continued WWT for up to 2 weeks.15
Moisturization: There are clear benefits of moisturizer application on skin hydration, either after bathing, or without bathing.16
Massage Therapy: In massage therapy, a licensed massage therapist often demonstrates the first few sessions so that the patient’s care provider can subsequently perform the technique at home. Massage can either be done in short (10 minute), daily sessions when done at home, or in longer, weekly sessions when performed by a licensed massage therapist.17 In one study, young children with AD were treated with standard topical care and massaged by their parents for 20 minutes daily for a 1-month period. A control group received standard topical care only. The children’s affect and activity level significantly improved, and their parent’s anxiety decreased immediately after the massage therapy sessions. Over the 1-month period, parents of massaged children reported lower anxiety levels in their children, and the children improved significantly on all clinical measures including redness, scaling, lichenification, excoriation, and pruritus. The control group only improved significantly on the scaling measure.18
Stress Reduction and Mindfulness: A randomized controlled trial compared the effectiveness of 4 group treatments for atopic dermatitis, a chronic skin disorder characterized by severe itching and eczema: dermatological educational program (DE), autogenic training as a form of relaxation therapy (AT), cognitive-behavioral treatment (BT), and the combined DE and BT treatments (DEBT). BT consisted of relaxation, self-control of scratching, and stress management. Group treatments were also compared with standard medical care (SMC). Assessments at 1-year follow-up showed that the psychological treatments (AT, BT, and DEBT) led to significantly larger improvement in skin condition than intensive (DE) or standard (SMC) dermatological treatment, accompanied by significant reductions in topical steroids used. The results corroborate preliminary reports that psychological interventions are useful adjuncts to dermatological treatment in atopic dermatitis.19 Additionally, the practice of mindfulness for patients with atopic dermatitis or other forms of chronic itch is not a substitute for well-tried coping strategies or medical therapy used so far, but can be integrated as an additional, valuable treatment option.20
Psychotherapy: Psychotherapy studies of AD patients report improvement in anxiety level and skin condition after psychotherapy. The results suggest that AD patients with a higher anxiety level are more likely to improve their psychological and dermatologic condition after psychotherapy but are more vulnerable to nonadherence when no adequate psychological treatment is offered. The results underscore the importance of proper psychological assessment and treatment in addition to dermatologic treatment.21
Patient/Parent Education: The need to provide information and advice was expressed strongly by patients in the 1990s. This led to the establishment of the “Ateliers d’Education à la Santé de la Peau” (Skin Health Education Workshops). These workshops, open to all patients, consist of an informative medical lecture, workshops dedicated mainly to hygiene, hydration, and alternatives to scratching, and relaxation. “Workshop” here means a collective experience, without a particular focus on the individual needs of each patient. The education program forms an integral part of a holistic therapeutic strategy: it is requested by doctors, but, above all, experienced as a need by patients.22
Consensus Recommendation
The value of treatments for patients with inflammatory skin conditions as well as post-cancer skin healing at the Hydrotherapy Center in Avène, France is well documented. While over 2000 patients undergo the 3-week intensive hydrotherapy treatment in France every year, the limitations of scaling the treatment to benefit the millions of patients living with inflammatory skin conditions23 is easily recognized. A panel of board-certified US dermatologists visited the hydrotherapy center to investigate the treatment protocols and review the scientific evidence supporting the therapeutic benefit of treatment with the low mineral thermal spring water with the unique biological signature identified by an original microorganism, Aquaphilus dolomiae, not yet described in other environments.9
The questions posed
Questions #1: Is there a clinical/therapeutic benefit for incorporating modified hydrotherapy treatments as an adjunctive treatment for inflammatory skin conditions?
The consensus was unanimous that modified hydrotherapy treatments would offer patients both alternative and adjunctive options for enhancing outcomes for patients with inflammatory skin conditions.
Question #2: How would hydrotherapy treatments be incorporated into dermatology practices?
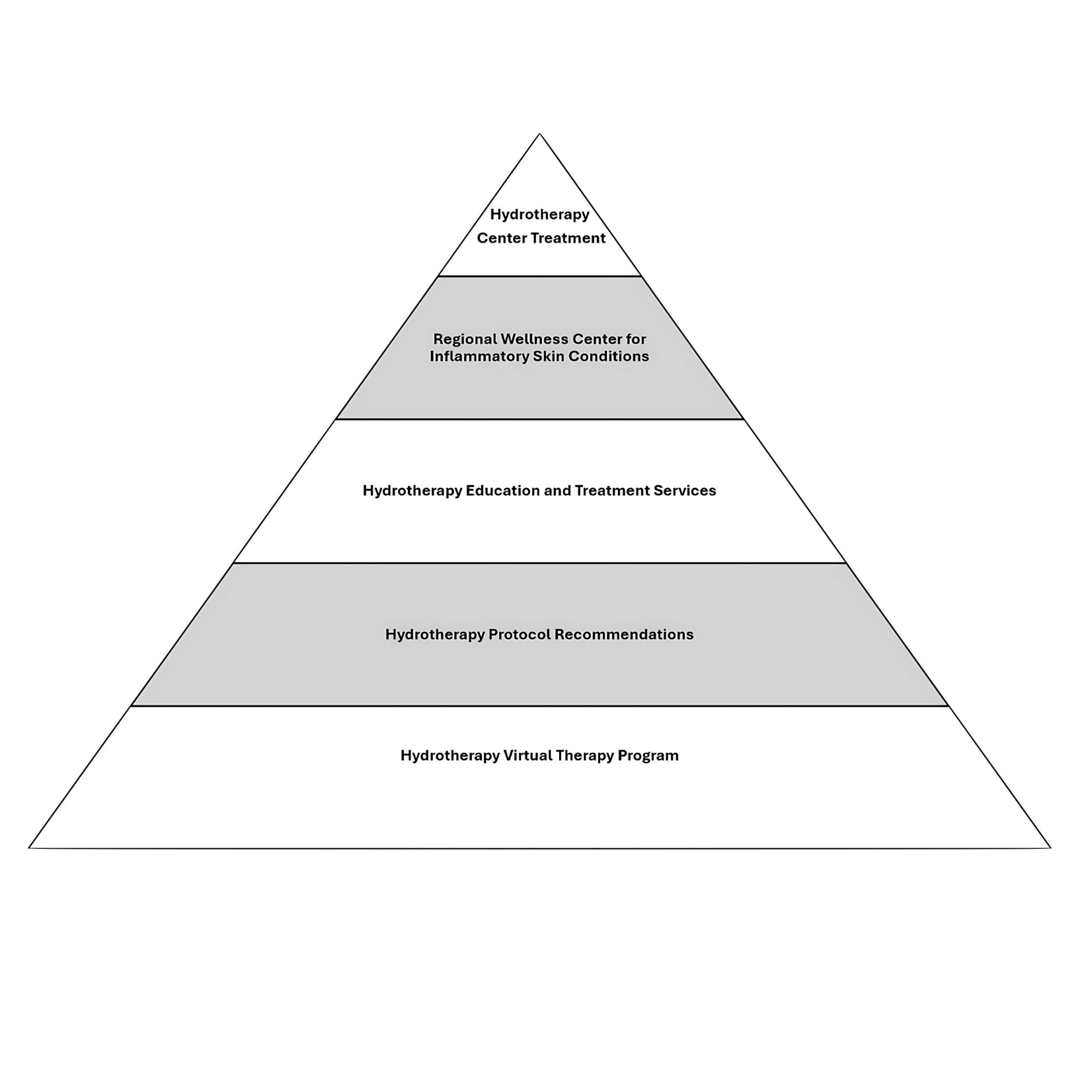
Dermatology business and patient treatment models differ significantly. A tiered approach was suggested to provide options for hydrotherapy treatments accommodating different practices and patient needs. (See Figure 1)
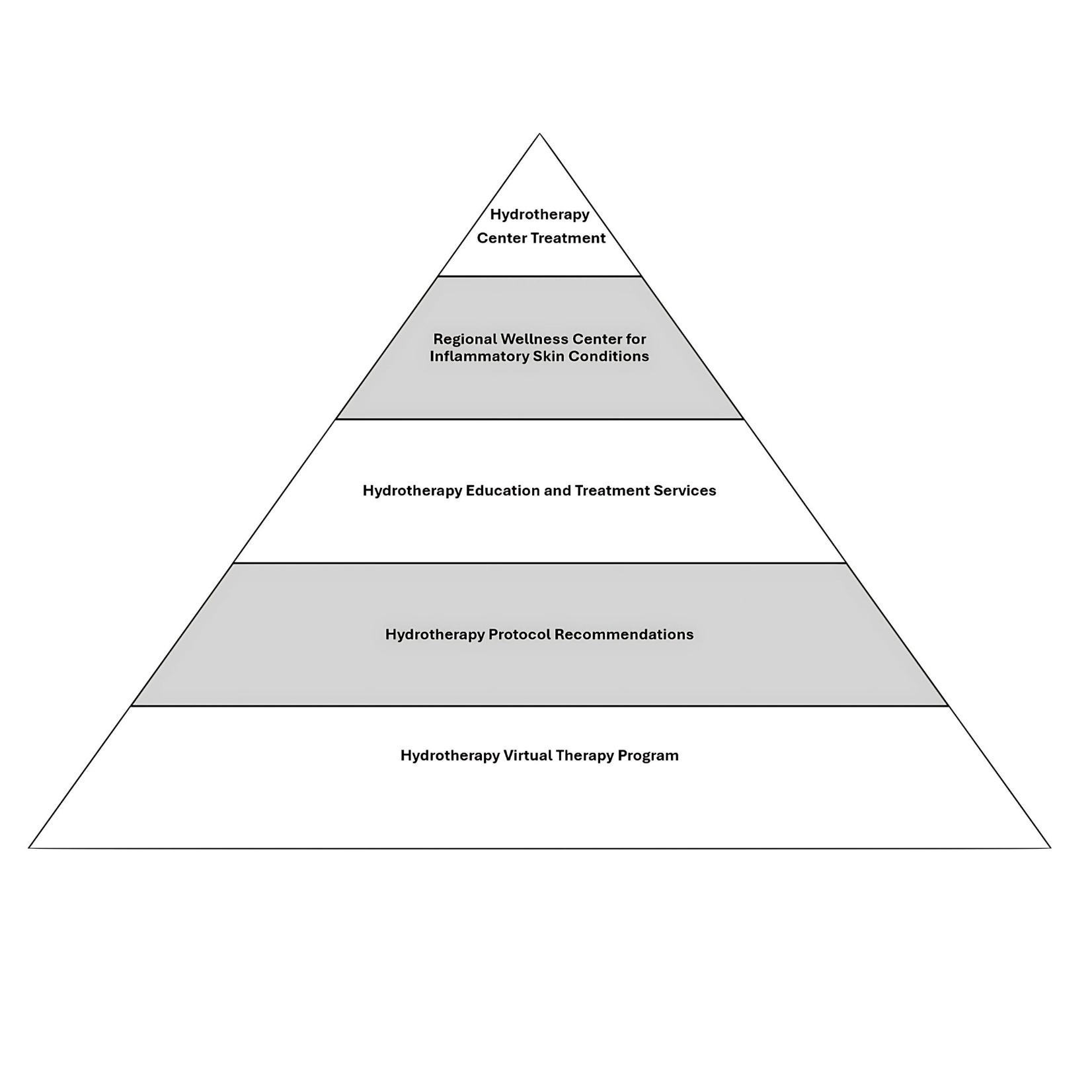
Sending patients to the Avène Hydrotherapy Center in France was not ruled out as the premiere solution. While logistically impossible and financially unfeasible for most patients, it was agreed that there is a patient population who would consider this treatment if informed of the option.
Regional Hydrotherapy Centers were considered as second tier option. These centers would offer face and body hydrotherapy treatments. Adjunctive services would include massage, modified wet-wraps, mindful/stress reduction strategies and psychotherapy. These centers would offer regular, high touchpoint treatments, patient education, home protocols, and workshops to reinforce integration of treatment into activities of daily living.
The third-tier recommendation is a single hydrotherapy treatment and education service. Patients would be coached on how to perform both body and facial treatments at home reinforced with virtual workshops.
The fourth-tier option is hydrotherapy treatment protocol recommendations utilizing digital/print support assets. Digital/printable assets and access to recorded educational workshops would be utilized.
The fifth-tier option is a hydrotherapy virtual clinic with pre-recorded training and interactive patient educational content.
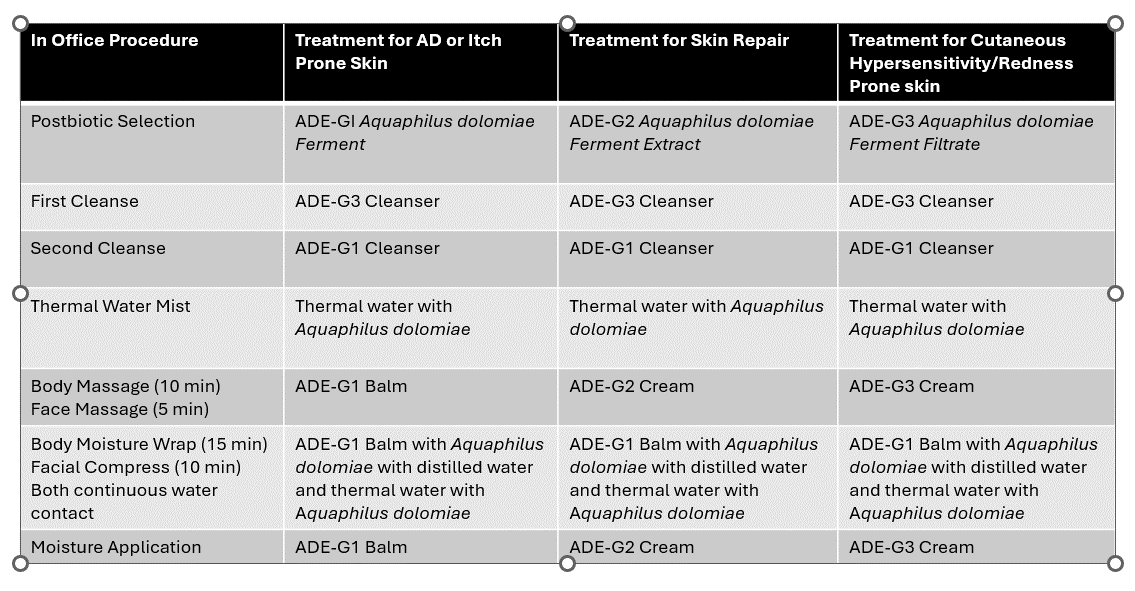
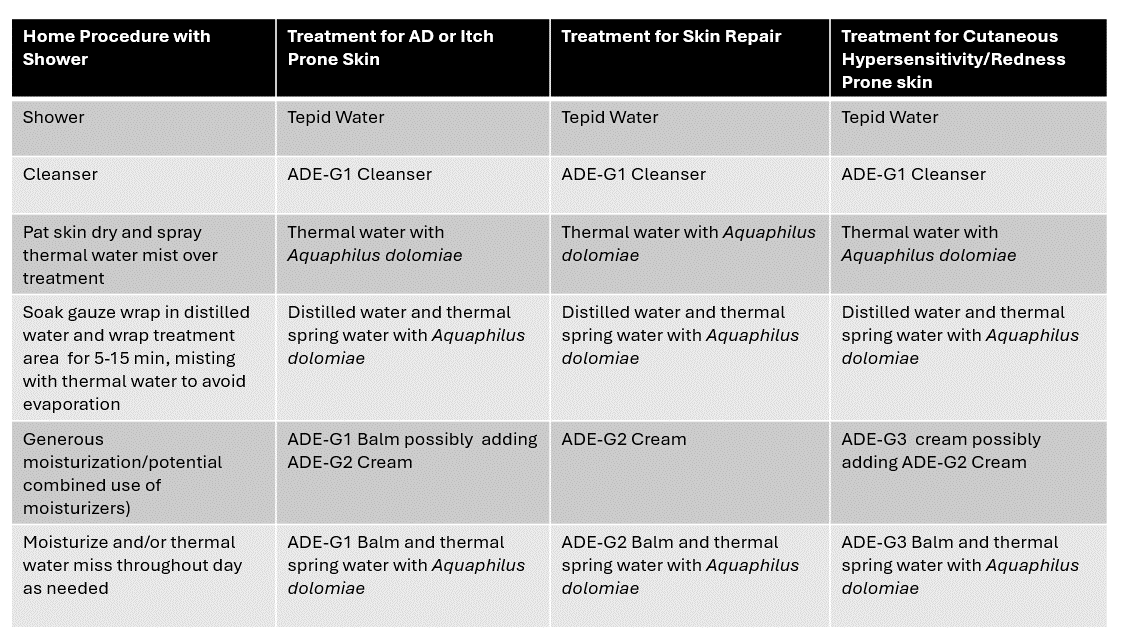
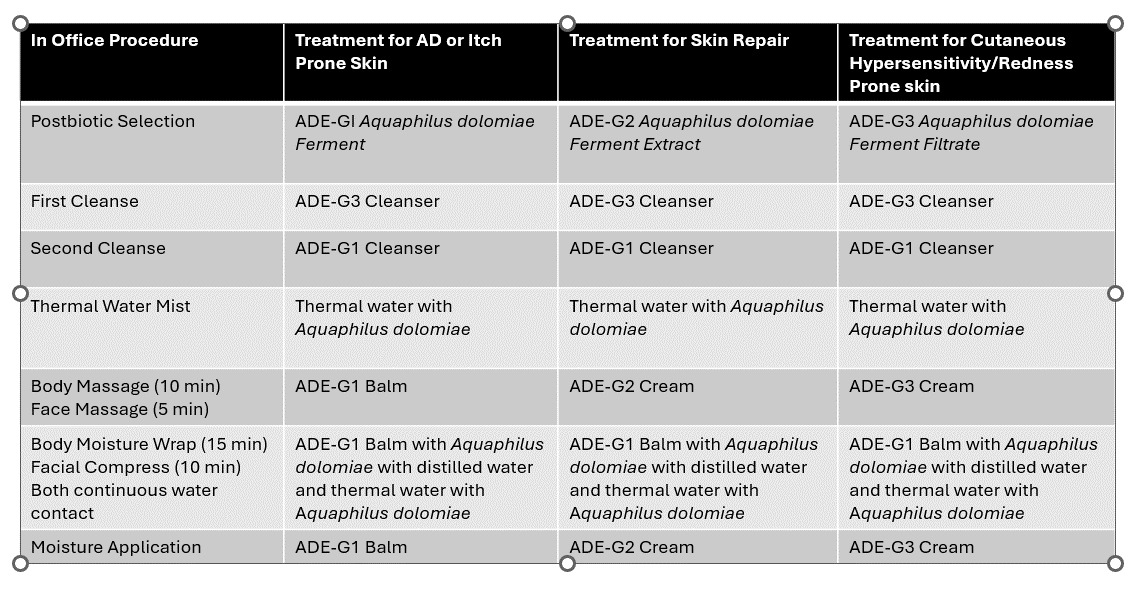
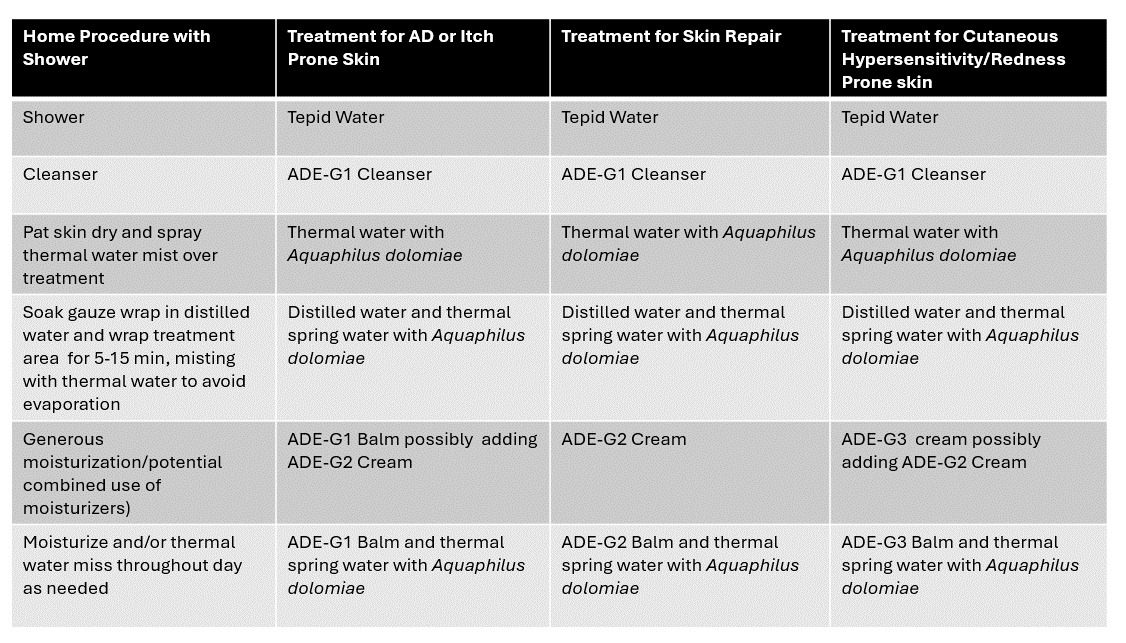
Question #3: To best emulate the hydrotherapy center treatment, what type of protocols would you consider?
The consensus positively agreed the hydrotherapy treatments could be modified for in-office procedures (Table 1) as well as at home therapy. (Table 2) These treatments would closely mimic the therapies performed utilizing both commercially available thermal spring water packaged in the retail cans and the postbiotic skincare products used in treatments at the center.
Conclusion
After evaluating treatment protocols and reviewing scientific literature, a panel of board-certified U.S. dermatologists visiting the Avène Hydrotherapy Center in France recognized the therapeutic potential of low-mineral thermal spring water, uniquely characterized by the microorganism Aquaphilus dolomiae. The panel reached a consensus on the clinical value of this modality and recommended exploring its emulation and integration into U.S. dermatological treatment protocols.
Disclosures
Dr. Lio reports being on the speaker’s bureau for AbbVie, Arcutis, Eli Lilly, Galderma, Hyphens Pharma, Incyte, La Roche-Posay/L’Oréal, Pfizer, Pierre-Fabre Dermatologie, Regeneron/Sanofi Genzyme, Verrica; reports consulting/advisory boards for Alphyn Biologics (stock options), AbbVie, Almirall, Amyris, Arcutis, ASLAN, Bristol-Myers Squibb, Burt’s Bees, Castle Biosciences, Codex Labs (stock options), Concerto Biosci (stock options), Dermavant, Eli Lilly, Galderma, Janssen, LEO Pharma, Lipidor, L’Oréal, Merck, Micreos, MyOR Diagnostics, Pelthos Therapeutics, Regeneron/Sanofi Genzyme, Sibel Health, Skinfix, Suneco Technologies (stock options), Soteri Skin (stock options), Theraplex, UCB, Unilever, Verdant Scientific (stock options), Verrica, Yobee Care (stock options). In addition, Dr. Lio has a patent pending for a Theraplex product with royalties paid and is a Board member and Scientific Advisory Committee Member emeritus of the National Eczema Association.
Dr. Sidbury reports investigator for Regeneron; Galderma; UCB; Castle; Pfizer. Consultant for Leo; Lilly; Arctutis; Dermavant; Micreos; Pierre Fabre. Speaker for: Beiersdorf.
Dr. Lal reports Dr. Lal reports consulting or speaker for AbbVie, Pfizer, Boehringer Ingelheim, Incyte, Sanofi, Arcutis, Sun Pharma, Lilly, Galderma, Avita, Sciton, Aerolase, Pierre Fabre, La Roche-Posay, CeraVe, Revision.
Dr. Golant reports consulting or speaker for Abbvie, Amgen, Arcutis, BMS, Dermavant, Galderma, Incyte, Janssen, LEO Pharma, Lilly, Pfizer, Regeneron, Sanofi.
Dr. Patel reports speaker agreements for Galderma, LEO Pharmaceuticals, Bristol Myers Squibb, Amgen.
Dr. Weinstein reports no disclosures.
Dr. Liu reports no disclosures.
Dr. Koh reports no disclosures.
Cheryl Barry reports employee, Pierre Fabre USA
Funding
This manuscript is supported by Pierre-Fabre, USA